Image Source: Pixabay
Image Source: Pixabay
Among the major issues not being discussed in the US presidential campaign are those facing the US healthcare system. The two main concerns are well-known.One is high cost. The US economy spends about $12,500 per person on health care in 2022, according to the OECD. The second- and third-highest countries, Switzerland and Germany, spend about $8,000 per person on health care. Canada is at about $6,300 per person, about half the US level. The United Kingdom is even lower at $5,600 per person. I’m not in favor of cutting US healthcare spending by half or more! But high and rising healthcare costs for government programs like Medicare and Medicaid are part of what makes forecasts for the US budget deficit so dire. And for those of us who get our health insurance through our employers, the high and rising cost of health insurance makes it harder to get increases in our paychecks, as well.The other main concern is the number of people who do not have access to health insurance. Census Bureau statistics suggest that 11% of working-age Americans (ages 19-64) and about 6% of children did not have health insurance in 2023. Many of these households fall through the cracks of the current system: they don’t have jobs that provide health insurance, and they have enough income that they may not qualify for Medicaid, but they don’t have enough income that paying for health insurance look affordable to them. Up to about half of the uninsured are actually eligible for health insurance at zero cost to them, whether private or public, but lack of knowledge and the administrative burdens of applying are too much for them.So what might be done? The Summer 2024 Journal of Policy Analysis and Management has a useful back-and-forth that identifies some possibilities, issues, and tradeoffs. On one side, Liran Einav and Amy Finkelstein summarize their arguments in a book they published in 2023 last year with their plan, called We’ve Got You Covered: Rebooting American Health Care. But redesigning the US health insurance system involves some big leaps, and as they acknowledge, their plan may be politically impractical. Thus, Jason Furman discusses the possibilities of more incremental–but potentially still important–health insurance reform. Here are links to the point/counterpoint:
The Einav and Finkelstein plan focuses on the idea of giving all Americans access to a basic level of health care at no charge to them. They argue that when other countries have included out-of-pocket cost-sharing for patients–say, co-pays, co-insurance, or deductibles–the other countries also end up having copious and often complex exceptions: say, for pregnant women, veterans, the unemployed, those with lower income levels, and so on and so on. Rather than create what can easily become an administrative swamp for cost-sharing, they would drop the idea of this basic level of care. They argue that “sharing in universal coverage is on a collision course with itself.”What would be included in this basic level of care? Linav and Finkelstein get a little fuzzy here, and start talking about “gray areas.”
Basic coverage must cover all essential medical care, including primary and preventive care, specialist care, and hospital care—both emergency and non-emergency. Much of what this means is obvious. Flu shots and appendectomies are in. Purely cosmetic plastic surgery is out. But there is also a large gray area of specific types of care where there are cases that can be made both for exclusion and for inclusion in basic care. Infertility treatment, dental care, vision care, physiotherapy, treatment of erectile dysfunction, various forms of long-term care—the list goes on and on. We deliberately do not weigh in here, other than to say that the starting point must be to define a budget for basic care—how much taxpayer money we are willing to devote to health care. Only then can we have a meaningful discussion about these gray area decisions. … [M]ost countries have a formal process for considering whether to cover new treatments under universal health care. We will need one too.
In addition to the question of what will be covered, there is also a question of how it will be covered. The social contract is about providing essential medical care, not providing a high-end experience. There are many non-medical aspects of care that may be desirable without being essential. The ability to see the doctor of your choice at your preferred timing and location, for example, or semi-private hospital rooms. This would be substantially limited under basic coverage. Basic coverage would likewise involve longer wait times for non-urgent care than what people with private health insurance or Medicare are currently accustomed to. Wait times would be closer to those experienced by Medicaid patients, or by veterans who receive their medical care through the Veterans’ Administration (VA).
Thus, the Einav-Finkelstein vision is that everyone would receive basic care through the same system, but they estimate that perhaps two-thirds of Americans would have supplemental insurance on top of that. To put it another way, employer-provided health insurance could pay part of the premium to the government to cover basic health care, and then the rest of the premium would be converted into top-up insurance.They argue that we could “fulfill our social contract without tackling the other multi-trillion-dollar elephant in the room: the problem of high and often inefficient healthcare spending. … Which is a relief, since we don’t (yet) have the silver bullet for dramatically lowering healthcare spending while fulfilling the dictate to “do no harm” to the patient. Nor, we hasten to add, does anyone
else. Despite what you may have heard on TV. It’s indisputable that there is a lot of waste in U.S. health care. But the old adage about advertising is also true: half of spending is wasted, we just don’t know which half.”Jason Furman was a top economic adviser to President Obama, and thus a supporter of the Patient Protection and Affordable Care Act of 2009, which reduced the number of those without health insurance by about 22 million, at an annual cost of more than $100 billion. But one political advantage of the legislation is that for many (not all!) people who had private or government health insurance, their avenues to health care were not much changed by the legislation.As Furman points out, it’s easier to generalize about “basic care” than to define it in detail. It’s hard to imagine a politically practical “basic care” system that includes less than Medicaid–and Medicaid already pays such low amounts that many healthcare providers refuse to take additional patients. How “basic” could “basic” be? And are Americans willing to tolerate “basic”? Furman notes:
As Einav and Finkelstein discuss at length, much of what is provided by the health system is “amenities,” which cost money and resources but do not contribute to better health outcomes. This distinction between the primary purpose and the amenities is rarely made in other spheres. For example, imagine a management consultant studying the $150 billion annually spent on hotel rooms in the United States. They might conclude that about $125 billion of that sum was wasted because hostels could have provided the same shelter, with a bed, access to toilet, and showers, at a much lower cost. But this recommendation would miss the point.
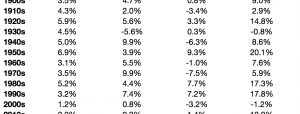
Furman argues for cost-sharing when it comes to healthcare expenses, on the grounds that people need to have some connection to what they are actually paying for healthcare because if they don’t do so, they aren’t likely to think about tradeoffs. He writes: “The financing of healthcare is already very opaque with a typical family of four spending about $32,000 annually but possibly only noticing the about $3,000 they pay out of pocket or maybe also the about $6,000 they contribute to the premium for their plan. The rest of the money is in the form of foregone wages (the incidence of the employer contribution for health insurance) and taxes for healthcare.”He points out that cost-sharing for health care expenses in some form is common across other countries. Indeed, the existing level for cost-sharing on health care, as a share of household consumption spending, is actually not that different in the US than in many other countries. Furman writes:
Furman writes:
One thing I learned from working on the ACA [Affordable Care Act] was that no one had all or even most of the answers, especially when it comes to delivery system reform … The answer is to take more seriously how to put in place systems and processes that can discover better answers over time, not simply assume that one knows them in advance—let alone knowing whether they will be politically or socially sustainable. …
But it is also wrong to ignore the fallibility of government or the people that implement its policies either. Medicare is a poorly designed insurance plan that would not even qualify as insurance under the ACA mandate because of its unlimited cost sharing (despite having first dollar coverage for many services), as a result it is basically unusable as a sole insurance plan—with 90% of beneficiaries
supplementing it with something else. It took the federal government decades to add a prescription drug benefit to Medicare, an omission that would have driven any private insurer out of business. And even when government plans have come in under cost, like the prescription drug benefit, a big part was because of innovations that were unanticipated or underestimated by the creators of these plans, like tiered formularies for prescription drugs.
I do not know the answer, but it should involve some of what is best about markets while remedying what is worst about them … It also needs to do what is best about the government while building in a process of innovation and change, something like the Center of Medicare and Medicaid Innovation Center. And the most vexing issues in healthcare are how to balance its cost against the many other desires and priorities people have—so a mechanism that makes costs and tradeoffs more transparent is essential to ensuring the competition and innovation process will lead to better results over time.
I don’t have a one-size fits all answer for how to fix the US healthcare system either. But I do think it’s important that people have a better sense of what health insurance actually costs. One proposal with cost estimates from the Congressional Budget Office would be to look at the range of employer-provided health insurance across employers, and figure out the median amount provides, which CBO estimates at “$8,900 a year for individual coverage and $21,600 a year for family coverage.” That median amount would continue to be excluded from taxation. But for health insurance plans costing more than this amount, the additional amount would be counted as income to the worker. The CBO estimates that this would raise more than $100 billion per year by 2027.More By This Author:A Surge In US R&D SpendingUS Productivity Growth: Downside, UpsideEverything You Want To Know About Inequality: The IFS Deaton Review